
Many are warning that “they’re coming for our children now” with regard to COVID-19 vaccine mandates. Further, some have reacted with indignation to Fauci having recently pointed out in support of such mandates that “it is not something new” to mandate vaccines for schoolchildren and that this has been done for decades. Their indignation is presumably based upon the belief that mandates for COVID-19 vaccines will be materially different from mandates for other vaccines already used in children.
In fact, Fauci, the reigning king of deceitful double-speak, actually got something right. Vaccines already mandated upon children are similar to COVID-19 vaccines in many respects, except not in good ways, as Fauci would have us believe.
Many assume that COVID-19 vaccines will be the first vaccines mandated upon children without a showing of necessity, and without rigorous safety testing. They also assume that they’ll be the first mandated upon them without proven, long-lasting efficacy. They’re wrong on all counts.
Many other vaccines have been mandated upon US children without proof of necessity, safety, or long-lasting efficacy.
In 1986, broad legal immunity was granted to the manufacturers of vaccines recommended by the CDC for use in children. Since that time, the number of doses and vaccines on the CDC’s childhood schedule has increased alarmingly.
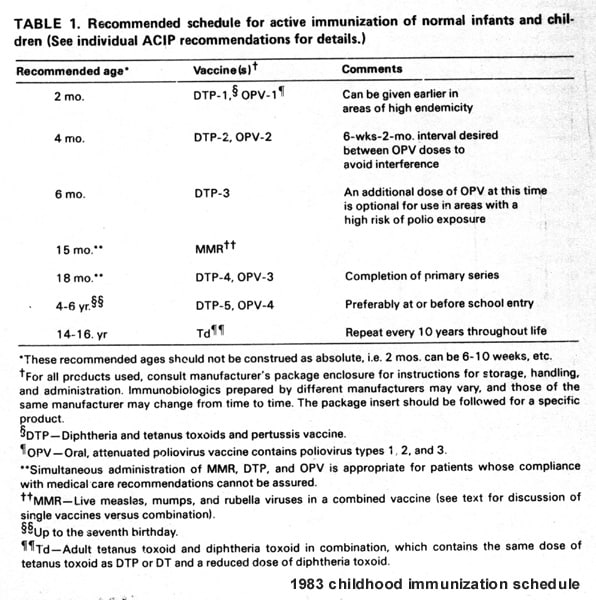
In 1983, the CDC recommended 24 doses of 7 vaccines by age 18. However, as explained in an August 19, 2021 article by Children’s Health Defense (CHD), “In the US, the vaccine schedule for children and adolescents currently includes as many as six dozen doses through age 18: up to 27 doses of 10 vaccines (14 antigens) through 15 months of age, another 13 doses of 8 vaccines (11 antigens) through age 18, plus one to two annual flu shot doses.”
{kind=link}
Many of these vaccines are mandated upon schoolchildren by state law and share disturbing aspects with COVID-19 vaccines. Below is a discussion of a few of them, to illustrate this point.
Newborns and infants are being administered a hepatitis B vaccine without proof of necessity, safety, or long-lasting efficacy.
The CDC recommends a hepatitis B vaccine at birth, 1-2 months of age, and 6-18 months of age. Nearly all states mandate the vaccine for school attendance.
Hepatitis B is not spread through casual contact. According to the CDC, it’s spread when blood, semen, or other body fluids from a person infected with the virus enters the body of someone who is not infected and this can happen through sexual contact; sharing needles, syringes, or other drug-injection equipment; or from mother to baby at birth.
In a January 31, 2019 article, CHD explained that “newborns are probably the least likely human beings on the planet at risk of actually getting hepatitis B” unless their mothers harbor the virus, and that this can be determined through routine prenatal blood testing. The article states, “In 1986 (five years before the CDC began pushing for vaccination of all newborns), the nation documented fewer than 280 cases of hepatitis B infection in children under age 14; by 2006, the Vaccine Adverse Event Reporting System (VAERS) had received over 23,000 reports of adverse events related to hepatitis B vaccination in the 0-14 age group, including nearly 800 deaths.”
CHD’s article also points out that the hepatitis B vaccine has been shown to wear off well before the age of any likely exposure to the hepatitis B virus.
Further, in November of 2020, the CDC conceded, in response to a request from the Informed Consent Action Network (ICAN) for “documentation sufficient to reflect any case(s) of transmission of Hepatitis B in an elementary, middle, or high school setting,” that it had not located any records pertaining to the request, meaning that it couldn’t find documentation of any case of hepatitis B transmitted in a school setting.
And, quite astoundingly, although children who are uninfected with hepatitis B but unvaccinated for it are barred from attending school in most states, children infected with the virus are permitted to attend school. This fact may be enlightening to those who believe that vaccine mandates first became illogical when COVID-19 came along.
Given the facts, it’s ludicrous to suggest that there is a medical necessity for universal vaccination of US babies against hepatitis B. Additionally, there has been woefully inadequate safety testing of the hepatitis B vaccines injected into them.
Of the two hepatitis B vaccines licensed by the FDA for injection into newborns, Merck’s was licensed based upon clinical trials which reviewed for adverse reactions for only five days after injection and GlaxoSmithKline’s was licensed based upon such trials which reviewed for them for only four days after it. This lack of rigorous safety testing is not unique among the childhood vaccines. For example, Merck’s Hib vaccine and Sanofi Pasteur’s polio vaccine were each licensed based upon clinical trials which reviewed for adverse reactions for only three days post injection.
A December 31, 2018 letter from ICAN to HHS contains an in-depth discussion of the shockingly short periods of monitoring for adverse reactions that occurred in the pre-licensure clinical trials for the childhood vaccines. It includes a table listing each vaccine and its corresponding disease, along with the “duration of safety review after injection” for each. The reader may want to sit down before viewing that table.
The monitoring for adverse reactions to childhood vaccines in the post-licensure period is also inadequate. VAERS, which is operated by HHS, is used to capture vaccine adverse events post-licensure, when the vaccines are already being administered in the population. However, HHS has long known that VAERS is highly inefficient at capturing adverse events. An HHS-funded study by Harvard Medical School tracked reporting to VAERS over a three-year period at Harvard Pilgrim Health Care and concluded in 2011 that “fewer than 1% of vaccine adverse events are reported.”
Refocusing on necessity, the hepatitis B vaccine is far from the only vaccine recommended by the CDC for children, and mandated upon children by state law, without proof of necessity.
Mythology about the accomplishments of vaccines in the US has caused false assumptions by the public about the necessity for them. In fact, death rates from infectious diseases had already plummeted in the US before the widespread use of vaccines, due largely to advances in the standard of living.
Despite this history, many assume that children were dropping like flies from infectious diseases such as measles, mumps, and chickenpox right before mass vaccinations began in the US, and that vaccines were our collective savior. In fact, they were not, on both counts.
There has been no showing of necessity for mass measles vaccination, and widespread use of the measles vaccine has altered a beneficial, natural pattern.
All states mandate the MMR (measles, mumps, and rubella) vaccine for schoolchildren.
Prior to the use of a measles vaccine, the annual death rate in the US from measles was low, at approximately 1 in 10,000 of those infected. Of course, not every American was infected with measles each year, so the overall annual death rate among the entire US population from measles was far lower than this.
With this low death rate, having measles in the pre-vaccine era was typically viewed as a benign childhood rite of passage. This is illustrated by the fact that the producers of the show The Brady Bunch made a humorous episode about the measles in 1969.
In the pre-vaccine era, a natural pattern had emerged whereby measles generally occurred within the group least likely to be harmed from it, children, and those more likely to suffer serious complications from it, infants and adults, were afforded protection from it. Unfortunately, widespread use of the measles vaccine has destroyed this natural pattern.
Before vaccine usage, only wild-type measles virus existed, and most people were infected with measles only once, during childhood. This one-time infection generally conferred lifelong protection from measles. Females infected with wild-type measles virus during childhood generally develop, and then pass to their infants, protective antibodies, in a process called passive immunity. This confers protection from measles during infancy. Vaccination interferes with this process, preventing the contraction of measles during childhood, and thereby affecting the level of passive immunity that mothers pass to their infants. Although some passive immunity is passed from mothers who were vaccinated during childhood to their infants, it is a less robust level than that passed by unvaccinated mothers infected during childhood with wild-type measles.
Failure of the measles vaccine’s effectiveness, combined with the vaccine’s interference with maternal passive immunity, has widened the age distribution of the infection, thereby increasing its incidence in those most at risk (infants and adults).
Further, the vaccine strain of measles can cause a condition with rash and fever which may be clinically indistinguishable from a measles infection. Approximately 5 percent of those receiving a measles vaccine experience this vaccine strain condition. For example, during the well-known 2015 California Disneyland outbreak, and in subsequent US measles cases that year, laboratory virus sequences were available for 194 of the cases and, of those, 73 (38 percent) were identified as vaccine strain sequences.
Widespread use of the measles vaccine has put the US on a problematic path, not rescued it from mass death and disability as we’ve been propagandized to believe. This story of opportunity costs, in terms of diminished natural protection, and of unforeseen consequences, may be ringing bells of recognition for those paying close attention to COVID-19 vaccines.
There has been no showing of necessity for mass mumps vaccination, and widespread use of the mumps vaccine has altered a beneficial, natural pattern.
Generally, mumps is relatively harmless when experienced in young children, who often exhibit no symptoms. However, when adolescents or adults have mumps, they’re more likely to experience serious effects, including inflammation of the brain, the membranes covering the brain and spinal cords, the pancreas, the ovaries, the parotid glands and the testicles. Further, having mumps as an adolescent male can cause orchitis, a condition that can cause infertility.
Due to ineffectiveness of the MMR vaccine, there has been an increase in the size and number of mumps outbreaks in highly vaccinated populations. Further, use of the vaccine has acted to postpone the onset of mumps, shifting it to older individuals who are at much greater risk of the complications discussed above.
There has been no showing of necessity for mass chickenpox vaccination, and widespread use of the chickenpox vaccine has altered a beneficial, natural pattern.
Nearly all states mandate chickenpox vaccination for schoolchildren.
Chickenpox is generally mild when experienced in childhood and, like measles, was historically viewed as a benign childhood rite of passage. Chickenpox and shingles both stem from the same varicella-zoster virus (VZV). Having chickenpox during childhood is associated with fewer risks than having it later in life, and with fewer risks than having shingles as an adult.
Two vaccines are used in the US for chickenpox: Varivax and ProQuad. These vaccines, and one vaccine used in the US for shingles, Zostavax, are made from live, attenuated VZV virus. One receiving a live virus attenuated vaccine can shed live virus, potentially spreading the virus to others. Measles, mumps, rubella, smallpox, chickenpox, zoster, yellow fever, rotavirus, and some flu vaccines use live attenuated viruses.
Before widespread use of the chickenpox vaccine in the US, children infected with chickenpox helped boost adults’ immunity to shingles by inhibiting the latent VZV’s reactivation in adults. However, there is evidence that the reduction in childhood chickenpox infections from use of the chickenpox vaccine is causing an increase in shingles cases, due to loss of this boosting effect. This impacts both children and adults, as explained in an April 25, 2019 article by CHD, which states,
Chickenpox and shingles infections both stem from varicella zoster virus—and before the advent of the varicella vaccine, children infected with chickenpox helped boost adults’ immunity to shingles by inhibiting the latent virus’s reactivation. Chickenpox vaccination disrupted this intergenerational protective mechanism, not only eliminating regular boosting for adults but shifting downward the average age at which shingles occurs. In addition , because varicella vaccine-induced immunity decreases by 8% with each year since vaccination, previously vaccinated young adults are at increased risk for varicella outbreaks and potential complications later in life. In short, while the reduced circulation of wild chickenpox virus may spare some healthy children a benign case of chickenpox, children now face the more serious risk of developing shingles at young ages and chickenpox at older ages.
From an inert-placebo control standpoint, COVID-19 vaccines are actually an improvement over vaccines already mandated upon children.
Some may assume that there cannot be any vaccines already mandated upon children with more glaring holes in their safety testing than COVID-19 vaccines. However, in one regard— the use of inert placebo controls—there are.
The definition of “vaccination” has repeatedly been revised to suit the needs of the CDC and the vaccine industry. To some extent, knowledge of this has reached the public in connection with COVID-19 vaccines, including via a September 8, 2021 tweet by US Congressman Thomas Massie.
However, many may not realize that the word “placebo” has also been churned through the Orwellian re-definition machine by those same players. The “placebo” given to control groups in vaccine clinical trials is often a non-inert substance, including another vaccine.
Vaccine safety trials are generally designed and conducted by vaccine manufacturers. Only one out of the approximately 30 vaccine brands routinely injected into US children was licensed based on a clinical trial which used an inert placebo in the control group. I again refer the reader to ICAN’s December 31, 2018 letter to HHS, as it contains extensive discussion of the use of non-inert placebos in clinical trials for vaccines used in children, along with tables identifying the non-inert substances given to the control groups for each vaccine.
For example, when Merck conducted clinical trials for its Gardasil 9 vaccine, it used the original Gardasil vaccine as the “placebo” in control groups, and both vaccines contain an aluminum adjuvant.
Fortunately, ICAN filed a petition with the FDA in June of 2020 demanding, among other things, that the FDA mandate that all clinical trials of COVID-19 vaccines use a true placebo control (a saline injection without anything added). Nine days after ICAN filed the petition, the FDA issued emergency guidance requiring that all COVID-19 clinical trials use such a control group.
However, despite this “safety victory,” vaccine manufacturers conducting COVID-19 vaccine clinical trials are engaging in a practice which prevents the existence of long-lasting, true comparator groups, because they are allowing participants who received placebos in the clinical trials to later receive COVID-19 vaccines.
The CDC has not proven that its entire schedule of recommended childhood vaccines provides a net benefit to children’s health, and unvaccinated v. vaccinated data indicates that unvaccinated children are healthier.
Most children receiving COVID-19 vaccines will receive them in addition to the staggering number of vaccines and doses already on the CDC’s childhood schedule. Just as the CDC hasn’t shown that COVID-19 vaccines would provide a net benefit to children, it hasn’t shown that its entire schedule of childhood vaccines provides a net benefit to them.
For decades, parents, doctors, and scientists have requested that the CDC conduct, or require, a long-term, properly controlled study comparing the health outcomes of unvaccinated and vaccinated children. Of course, those in favor of vaccinating children and who are confident that doing so makes them healthier should welcome such a study. To date, this request has gone unfulfilled.
Despite the CDC’s lack of action in this area, recent studies have been conducted without its involvement which have produced alarming results, indicating that unvaccinated children have better health outcomes than those who are vaccinated. Several are discussed below.
A 2012 study compared children receiving an influenza vaccine with those receiving a saline injection and, although both groups had the same rate of influenza, the group receiving the influenza vaccine had significantly increased rates of non-influenza infections.
A study published in April of 2017 comparing 650 vaccinated and unvaccinated homeschooled children in the US found that, compared to completely-unvaccinated children, fully-vaccinated children had increased risks for allergies, ADHD, autism, eczema, learning disabilities, and neuro-developmental delay. Additionally, fully vaccinated-pre-term infants were found to have an increased risk for neurodevelopmental disorders compared to completely unvaccinated preterm infants.
A study published in November of 2020 using data from the practice of Dr. Paul Thomas, an Oregon pediatrician, found that the unvaccinated children born into his practice appeared to be significantly more healthy than the vaccinated children. The study is a retrospective analysis of the health records of approximately 3,300 children, covering a period of about ten years, comparing the health outcomes of the children (unvaccinated v. vaccinated to varying extents). It found that the vaccinated children were diagnosed with a broad range of conditions at much higher rates than their unvaccinated counterparts. It also found that the vaccinated children saw a doctor markedly more often than the unvaccinated children. Jeremy R. Hammond’s book, The War on Informed Consent: The Persecution of Dr. Paul Thomas by the Oregon Medical Board, discusses the study in depth, as well as the retaliation and censorship that Dr. Thomas has endured as a result of raising vaccine safety concerns.
Many other vaccines have been mandated upon US children without proof of necessity, safety, or long-lasting efficacy, but this doesn’t warrant mandating more vaccines upon them under the same circumstances. It warrants rescuing them from those already mandated.
Americans are watching the CDC push COVID-19 vaccines upon children in the clear absence of a showing of their necessity, safety, and long-term efficacy. As illustrated above, this is just more of the same bad behavior by the CDC. It’s just worse by degree than its prior conduct with regard to childhood vaccines. Fortunately, its conduct is no longer flying under the public’s radar. Now that the public is awakened, it should rescue its children from the entire gauntlet of vaccines already mandated upon them when protecting them from forced COVID-19 jabs.
from Fauci Actually Got Something Right, But for the Wrong Reasons